INTRODUCTION
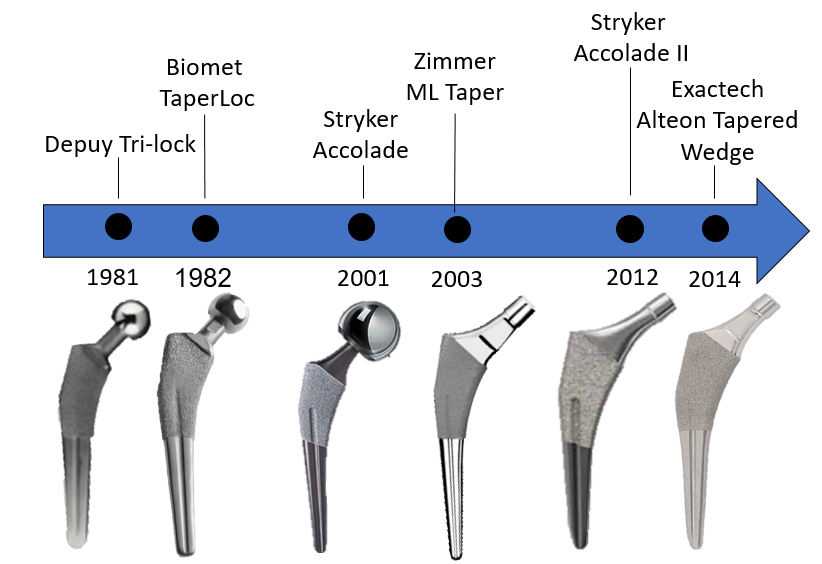
The single-taper wedge stem design is derived from the cemented Mueller stem of the 1970s. Unlike fit-and-fill stems, which contact most of the metaphysis, tapered wedge femoral stems are designed to achieve proximal medial/lateral fixation. Wedge femoral stems used in total hip arthroplasty (THA) have evolved from first-generation implants such as the DePuy Synthes® TRI-LOCK®, Biomet® Taperloc®, Zimmer® ML Taper, and Stryker® Accolade (Figure 1). These stems typically featured longer geometries and more robust distal shape. Continuing with the evolution, stems became shorter in length, had reduced distal geometries, and sometimes incorporated modular necks.
These first-generation designs have shown great clinical success with some studies reporting over 98% survivorship at 10 years.1,2,3 Despite this clinical success, a subset of the proximally-coated tapered wedge stems were failing to achieve stability and osteointegration. Cooper et al. retrospectively reviewed 320 tapered wedge femoral stems in non-cemented THA concluding that greater attention should be paid to femoral canals with a proximal-distal mismatch as well as stems that fill the canal in the mid- and distal-third of the stem.4 In an effort to reduce the occurrence of distally potted tapered, proximally coated wedge stems, the Alteon® Tapered Wedge Stem evaluated in this study was designed with a further reduced distal geometry. This design change is intended to provide a wedge-fit within the metaphysis of the proximal femoral canal for all femur types (Dorr A, B, C). The objective of this study was to evaluate the early clinical outcomes of the Alteon Tapered Wedge Stem (Figure 2).

METHODS
Three hundred and eighteen (318) subjects (163 males, 152 females and 3 not reported; mean age: 63.3±10.5 years; mean BMI: 28.1±6.0) underwent primary THA with a tapered wedge femoral stem. Subjects were enrolled in CR11-003 (“A post-Market Domestic (US) and International Data Collection to Assess Hip Replacement Systems Manufactured and/or Distributed by Exactech”) or CR14-001 (“Exactech Alteon Tapered Wedge Femoral Stem Total Hip Arthroplasty”). IRB approval was received prior to conducting the studies and all participants signed the informed consent. Clinical data outcomes for these studies included the Harris Hip Score (HHS), the Oxford Hip Score (OHS) and revisions. Weight-bearing A/P radiographs were reviewed by an independent third party at all post-operative time points for the patients enrolled in CR14-001. During this review, subsidence was measured by an independent radiology core laboratory using femoral stem features to measure the distance to bone features. Subsidence was noted if the change in position was greater than 5mm. Student’s t-tests were used to identify significant mean differences between genders (p<0.05).
RESULTS
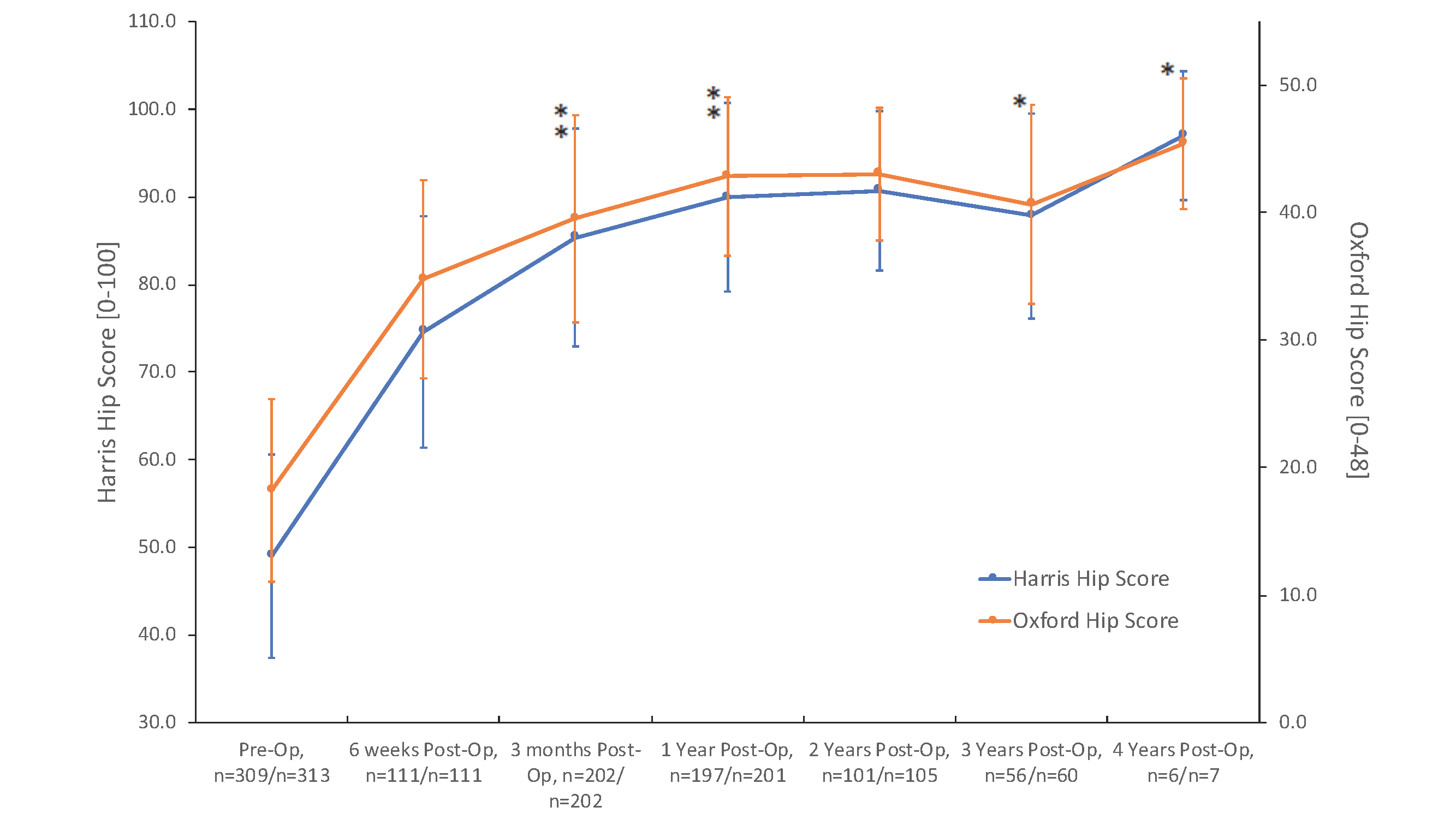
The means and standard deviations for the HHS and OHS are shown (Figure 3). For patients returning for their 2-year post-operative visit (n=101), the HHS improved by 41.7 points to 90.7 from 49.0, and the OHS improved by 24.8 points to 43.0 from 18.2. There was no significant difference between genders with regard to age, BMI or pre-op HSS scores. However, the males had significantly higher pre-operative OHS scores, 3-month, 6-month and 1-year post-operative HHS and OHS scores and 2-year post-operative OHS scores. There was a total of eight (8) revisions. Three were revised due to infection and the others were for instability, fracture, acetabular loosening, pain and periprosthetic fracture. There were no observations of subsidence at 1 year (n=45) or 2 years (n=40).
DISCUSSION
This tapered wedge stem exhibited positive early clinical results as demonstrated by the significant improvement in functional outcome scores from the pre-operative visit to 2-years post-operative. These 2-year improvements are better than the moderate clinically important improvements reported in the literature (40.1 points for HHS).5 Functional outcomes scores continued to improve at the 6-week, 3-month, 1-, 2- and 4-year post-operative visits.
There were no reports of subsidence at the 1- or 2-year post-operative time points for the radiographs examined by the third party. Jacobs and Christensen reported “significant progressive subsidence” between the 6-week and 1-year post-operative follow-ups of patients with the first generation cementless wedge stems. In their study, they reported that at 6 weeks 3 out of 130 hips showed signs of subsidence which then increased to 13 hips at the 1-year follow-up.6
Fifteen patients in the cohort that had their radiographs examined by the third party showed evidence of non-progressive radiolucent lines in the distal femoral component that were less than 2.2mm at 1 year. The low subsidence rates of the Alteon Tapered Wedge Stem indicate that the stem achieved good initial and short-term fixation, possibly due to the reduced distal geometry.
SIGNIFICANCE
The tapered wedge stem evaluated in this study demonstrated positive early clinical performance with no reports of subsidence. This tapered wedge stem design is a promising alternative to conventional femoral stems.
REFERENCES
- Healy W, Tilzey J, Lorio R, Specht L, Sharma S. Prospective, Randomized Comparison of Cobalt Chrome and Titanium Trilock Femoral Stems. J Arthroplasty. 2009;24:831-6.
- Burt C, Garvin K, Otterberg E, Jardon O. A Femoral Component Inserted without Cement in Total Hip Arthroplasty. J Bone Joint Surg Am. 1998 Jul;80(7):952-60.
- Lettich T, Tierney M, Parvizi J, Sharkey P, Rothman R. Primary total hip arthroplasty with an uncemented femoral component: two- to seven-year results. J Arthroplasty. 2007 Oct;22(7 Suppl 3):43-6.
- Cooper H, Jacob A, Rodriguez J. Distal Fixation of Proximally Coated Tapered Stems May Predispose to a Failure of Osteointegration. J Arthroplasty. 2011;26:78-83.
- Singh J, Schleck C, Harmsen S, Lewallen D. Clinically important improvement thresholds for Harris Hip Score and its ability to predict revision risk after primary total hip arthroplasty. BMC Musculoskelet. Disord. 17, (2016).
- Jacobs, Christensen. Progressive Subsidence of a Tapered, Proximally coated femoral stem in total hip arthroplasty. Int Orthop. 4:917, 2009.